RYLA APPLICATION AND CODE OF CONSENT
PLEASE:
1) COPY/PASTE THE WHOLE TEXT TO WORD,
2) FILL OUT AND SIGN
3) SUBMIT THE FORM SOONEST!!!
THANK YOU!!

PEACE CONFERENCE: LEADERSHIP AND PEACE
THROUGH CULTURAL DIVERSITY
FEBRUARY 14 – 17, 2013
RYLA REGISTRATION FORM
SPONSORING ROTARY CLUB:_____________________________________________________________
Email: _________________________________________ Phone#: ____________________________
NAME APPLICANT: _____________________________________________________________
Address: _____________________________________________________________________________
_____________________________________________________________________________________
Date of Birth: ____________________________________
NAME PARENTS: _____________________________________________________________
Mobile Phone : __________________________________
Email: _________________________________________ Phone#: ____________________________
NAME SCHOOL : _________________________________________
Address: _____________________________________________________________________________
_____________________________________________________________________________________
Phone#: ____________________________
IN CASE OF EMERGENCY, CONTACT:
NAME: ______________________________________________
Address: _____________________________________________________________________________
_____________________________________________________________________________________
Phone #:____________________________________
Describe briefly your reasons for applying for this RYLA PEACE CONFERENCE
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________
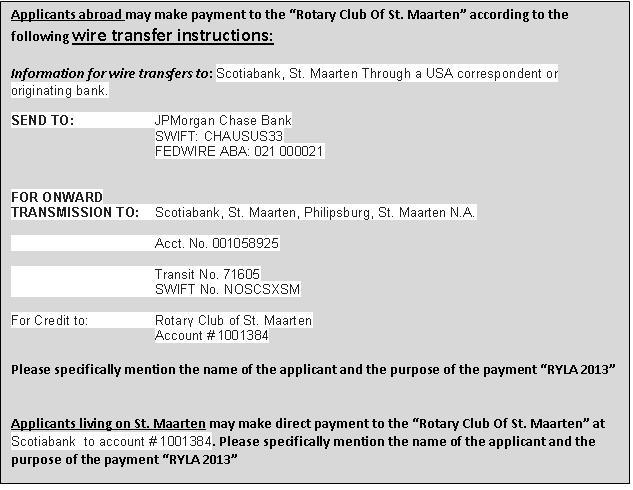
Registration Fee US$ 150 and must be paid no later than February 5, 2013.
Flight Arrival Information: Date dd/mm/yy ;Time _____AM/______PM; Airline &Flight #___________
Flight Departure Information: Date dd/mm/yy ;Time _____AM/______PM; Airline &Flight #_________
Signature of Parent granting permission: _____________________________ Date:_________________
Signature of Applicant:________________________________ Date:______________________
CONSENT, WAIVER & MEDICAL RELEASE FORM
Name of Sponsoring Rotary Club________________________________________
Student’s Guardian: Please print legibly on this form and return in registration packet
Name _________________________________Sex ______ Grade ________ Age ______
Address_________________________________________________________________
________________________________________________________________________
High School:_____________________________________________________________
Parent/Guardian Name(s):__________________________________________________
Address_________________________________________________________________
________________________________________________________________________
Home Phone # (______)_________________ Cell # (_____)_____________________
Family Physician’s Name ______________________Phone # (_____)_______________
Name of Primary Insurance Policy ___________________________________________
Date of last Tetanus shot ________________ Allergic to Tetanus Booster? ________
Participant Had:
Appendix Removed ________ Medical Authorization
Fainting Spells ________ Is participant taking any medication
Asthma ________ that must be given?____________________
Heart Trouble _________ If yes, please fill out below:
Convulsions ________ Medication: _________________________
Diabetes __________ Dosage _____________ Time ___________
Allergies to food or medicine? Activities to limit:_____________________
Specify: _________________ ____________________________________
Any other allergies?
Specify: _________________
Other (i.e. recent traumatic injury)
I consent to ______________________________(hereinafter “my child”) participating in RYLA. My child has permission to engage in all prescribed activities, except as noted above by me.
I also hereby authorize any medical treatment required by my child while in attendance at this event. I have described above any special medical or other needs required by my child, and will notify event personnel of any special needs or information required by my child.
Parent/Guardian Name:______________________________Relationship: ___________
Parent/Guardian Signature: ________________________________________________
Other person to notify in case of an emergency_________________________________
Other emergency phone (______) _____________________